Hepatic Encephalopathy (HE) is a deterioration in brain function developing in patients with acute liver failure or chronic liver disease. The brain is a very sensitive organ and relies on a healthy liver in order to properly function.
Classification
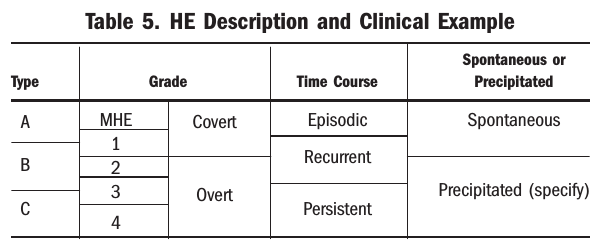
Type A is HE associated with Acute liver failure. Acute liver failure is a rapid deterioration (within days and weeks) of liver function in a person who had no pre-existing liver disease.
Type B is HE associated with portal-systemic Bypass without intrinsic liver disease. This occurs when blood flows “around” the liver and therefore the liver cannot control/remove substances in the blood. Type B usually occurs as a result of congenital abnormalities and/or as a result of an invasive procedures or trauma (such as a portosystemic shunt).
Type C is HE associated with Cirrhosis. Cirrhosis is a late stage of chronic liver disease when scarring (severe fibrosis) develops.
Classification de l'EH
Stade
Symptoms and signs of HE vary from mild to severe. In the mild stage of HE, called minimal HE (MHE) or covert HE (CHE), a person’s ability to carry out daily tasks (working, driving, sleeping at night) is affected and as a result leads to poor quality of life. A person suffering from MHE may experience anxiety, problems concentrating, poor memory or be unable to think clearly. A person with severe HE or overt HE (OHE), experiences impaired mental and neuromotor functioning (tremor of the hand when wrist is extended called asterixis) with obvious signs of mental confusion, gross disorientation, drowsiness and coma.
Covert HE
Grade 0: Minimal HE
Medical definition: Psychometric or neuropsychological alterations of tests exploring psychomotor speed/executive functions or neurophysiological alterations without clinical evidence of mental change.
This stage is very hard to detect as changes in memory, concentration and confusion are not so obvious for a healthcare provider to diagnose.
Grade 1:
Medical definition: Trivial lack of awareness, anxiety, shortened attention span, inability to add and subtract, altered sleep rhythm.
Patients have a short attention span and restlessness. They notice mood changes like depression, anxiety or irritability. They experienced poor night time sleep with daytime sleepiness.
Overt HE
Grade 2:
Medical definition: Lethargy or apathy, disorientation for time (naming day of month, month of year, season etc.), obvious personality change, inappropriate behavior, clumsiness, flapping tremor (asterixis).
Patients may notice they keep forgetting things, have no energy, and exhibit inappropriate behavior. Speech may be slurred and trouble doing mental tasks such as basic math could be seen. Hands might shake, creating difficulty to write. Patients experienced disorientation for time and space.
Grade 3:
Medical definition: Somnolence to semi-stupor but responsive to stimuli, confused, gross disorientation, bizarre behavior.
Confusion is installed : impossibility to say where you are or what day it is. Patients are extremely sleepy. They may not be able to do basic mental tasks. They may feel extremely anxious and act strangely (e.g. fits of rage, paranoia).
Grade 4:
Coma: when the person is unconscious and unresponsive to painful stimuli. There is a high mortality rate for people who go into a coma.
Timecourse
HE could be episodic, recurrent or persistent. This categorization refers to clinical symptoms experienced. For example, in case of episodic HE, a patient suffering from MHE will endure ponctual, overt symptoms. Recurrent HE is define as bouts of HE that occur with a time interval of 6 months or less. Finally, persistent HE is the opposite : a continual course of HE symptoms with scattered relapses.
Precipitants
The following triggers (precipitating factors) can cause or worsen HE:
Infections
Constipation
Dehydration
Bleeding inside intestines, stomach or esophagus (the tube connecting mouth to stomach)
Medications affecting nervous system such as sleeping pills, antidepressants or tranquilizers
Kidney problems
Alcohol use
Surgery
Having a portosystemic shunt. This surgical procedure is called TIPS (trans intrahepatic portal-systemic shunt), and is done to reduce the pressure built up in the portal vein (the vein entering the liver from the intestines). The procedure involves placing a small tube through liver to allow the blood to pass through liver (like a tunnel through a mountain) and therefore reduce the portal hypertension and associated complications (variceal bleeding and its management)
Diagnosis
HE is diagnosed through symptoms. Some symptoms are evident (OHE) and some are not so obvious (CHE) which may require taking a neuropsychiatric test. Those tests involve mainly to test cognitive abilities or motor coordination. Many tests exists :
Psychometric Hepatic Encephalopathy Score (PHES) : A collection of 5 different tests paper-pencil. For example, the patient is asked to link numbers or decipher symbols within a certain limit of time.
Stroop : This phone application is a technologic conversion of a test firstly described by John Ridley Stroop in 1935. This test involves pressing on the color of the words, which some are themselves the color’s names (which must therefore be ignored).
Inhibitory Control Test (ICT) : The patient have to responds to target letters (such as X and Y) and not to lures (non X and Y targets) and we measure the reaction time.
Electroencephalogram (EEG) : Electrodes detects activity of the brain.
Clicker Flicker Frequency (CFF) : A light is pulsing at various frequencies and patients have to indicates at which moment its flickering.
Impact for patients and relatives
Hepatic encephalopathy is often under-diagnosed, mainly his minimal form. This documentary show us what 4 patients are enduring day-to-day.
Référence
Hendrik Vilstrup, Piero Amodio, Jasmohan Bajaj, Juan Cordoba, Peter Ferenci, Kevin D. Mullen, Karin Weissenborn, Philip Wong (2014) Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology, 60: 715-735. doi: 10.1002/hep.27210